Most people with tuberculosis who are identified through community health surveys report no cough — the single symptom that public-health systems have historically relied upon to flag and isolate infectious patients. That finding, drawn from an analysis of national health data and discussed widely among infectious-disease researchers, is quietly reshaping how scientists think about one of the world’s oldest and deadliest bacterial diseases.
A Finding That Changes How We Think About TB
Tuberculosis kills approximately 1.3 million people every year, according to the World Health Organization — a toll that persists despite decades of established treatment. One reason containment remains so difficult may now be clearer: a meaningful share of transmission appears to occur before, or even without, the visible symptoms that prompt people to seek care and that contact-tracers use to identify dangerous spreaders.
The scale of TB’s contagiousness under ordinary circumstances is already striking. A single untreated person with active tuberculosis can infect between 10 and 15 others, according to established epidemiological data. That transmission rate becomes considerably harder to contain if the most infectious individuals do not yet know — or show signs — that they are sick.
A new study covered by science outlets including Earth.com warns that people with asymptomatic tuberculosis may be sustaining chains of community transmission that current public-health surveillance is structurally not designed to catch. Researchers are careful to note that this does not rewrite TB science from scratch. It does, however, sharpen an urgent question: how much of the global TB burden is seeded by people who feel completely fine?
How Tuberculosis Actually Travels Through the Air
Understanding why presymptomatic spread is plausible requires understanding how TB moves between people. The bacterium responsible, Mycobacterium tuberculosis, travels through the air inside microscopic respiratory particles called droplet nuclei. These particles are so small and light that they can remain suspended in indoor air long after the person who exhaled them has left the room.
According to the U.S. Centers for Disease Control and Prevention, TB germs enter the air when someone with active TB disease coughs, speaks, or sings. Unlike larger respiratory droplets that fall quickly to the floor, droplet nuclei carrying Mycobacterium tuberculosis can drift across an enclosed space and be inhaled by someone who never came face-to-face with the source person.
That said, tuberculosis is notably less contagious than COVID-19 or influenza. Catching TB generally requires sustained proximity to an infectious individual — typically sharing an indoor space over hours or days — rather than a brief passing encounter. Transmission in open, well-ventilated environments is rare. These characteristics matter for putting the presymptomatic-spread concern in appropriate context: this is not a disease that spreads from a single shared elevator ride.
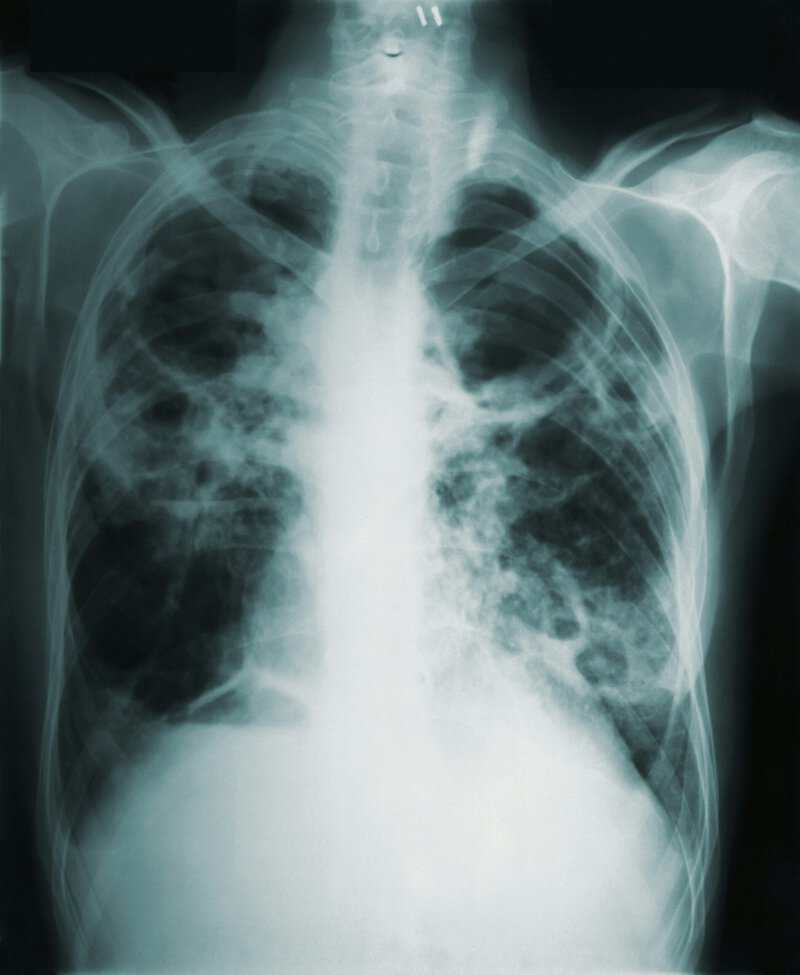
Once inhaled, the bacteria travel deep into the lungs. In roughly 90 percent of exposed individuals with healthy immune systems, the body’s defenses contain the bacteria in a dormant state known as latent TB infection — a condition that produces no symptoms and is not contagious, but can reactivate into infectious active disease months or even years later, according to the Mayo Clinic.
Presymptomatic vs. Asymptomatic TB: An Important Distinction
Active TB disease — the infectious stage — is classically associated with a persistent cough lasting three or more weeks, night sweats, unexplained weight loss, and low-grade fever. But the disease does not always present so clearly, particularly in its earlier phase, and the scientific community is increasingly distinguishing between two phenomena that the new research brings into focus.
Presymptomatic spread refers to transmission that occurs during the window between when a person becomes infectious and when they develop noticeable symptoms. This concept is well established with influenza and COVID-19, but has only recently been examined rigorously in the context of tuberculosis, where incubation and progression timelines are far longer and more variable.
Asymptomatic TB, by contrast, describes active infection without symptoms that may persist indefinitely in some individuals. Researchers now recognize that tuberculosis patients who feel entirely fine can be nearly as infectious as those with overt, classical symptoms — a conclusion that, if replicated in larger prospective studies, would have significant implications for how screening programs are designed.
Scientists caution that not every asymptomatic person with TB is equally infectious. Bacterial load, immune response, and the specific pattern of lung pathology all mediate how readily the disease transmits from one person to another. Blanket conclusions about asymptomatic spread being universally as dangerous as symptomatic spread are not supported by current evidence.
What the New Study Found — and How Researchers Got There
The analysis combined contact-tracing data, molecular epidemiology — specifically, DNA fingerprinting of TB strains to map transmission chains — and self-reported symptom surveys gathered from national health programs. This multi-method approach strengthens the credibility of the conclusions by triangulating findings across independent data sources rather than relying on any single line of evidence.
The central finding was that the majority of community-identified TB cases reported no cough at the time of diagnosis. Because cough has long served as the primary red flag in both clinical and public-health settings — the symptom that prompts testing, triggers contact investigations, and guides isolation decisions — its absence in most identified cases directly challenges the assumption that symptomatic screening captures the most dangerous spreaders.
Asymptomatic individuals were found to be contributing meaningfully to ongoing transmission clusters, not merely serving as passive reservoirs of infection that rarely spill over to others. Scientists involved in the research stressed, however, that the findings represent an emerging pattern rather than settled consensus. They called for larger prospective studies — those that enroll participants before disease progression and follow them forward in time — to quantify the precise contribution of presymptomatic and asymptomatic spread to overall TB burden.
The Gap in Global TB Control
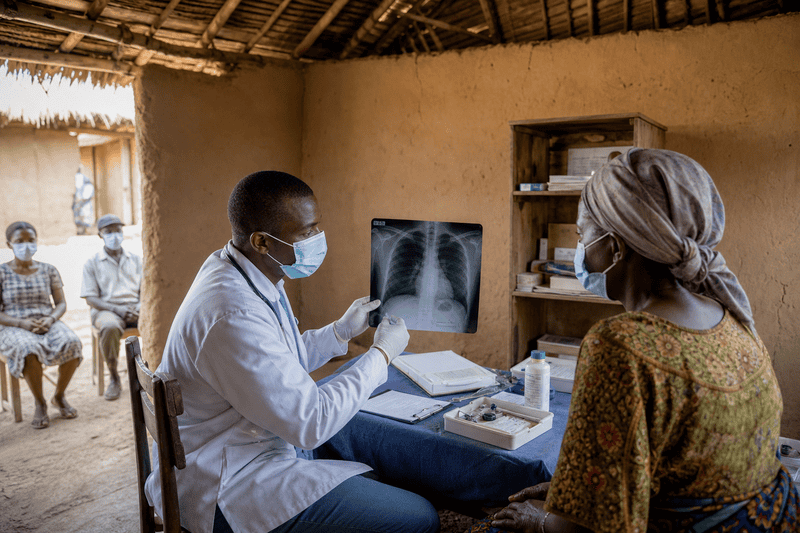
The implications for public health are significant. Current WHO-endorsed TB control strategy relies heavily on identifying and treating symptomatic patients quickly — a framework built on the foundational assumption that the most infectious people are also the most visibly unwell. If a substantial proportion of transmission occurs before or without symptoms, passive case-finding — waiting for sick people to feel ill enough to seek care — may be systematically missing a reservoir of spread.
Active community screening, which proactively tests populations rather than waiting for symptomatic patients to present at clinics, could in theory address this gap. But the populations that bear the greatest TB burden are predominantly in low- and middle-income countries where widespread asymptomatic screening is logistically and financially difficult to implement at scale.
Experts not involved in the study noted that these findings add scientific weight to longstanding advocacy for universal TB screening programs in high-burden settings. They cautioned, however, that implementation raises complex questions of cost, health-system capacity, and equity — particularly regarding who bears the burden of expanded surveillance and who benefits from it. Tuberculosis outbreaks continue to be reported even in higher-income settings; UChicago Medicine reported on a notable U.S. outbreak in early 2025, underscoring that the disease is not solely a problem of the developing world.
Putting Risk in Perspective: What This Does Not Mean

The presymptomatic-spread findings should not be read as a signal that tuberculosis has become an ambient, unavoidable environmental hazard. Several important constraints on TB transmission remain firmly in place and are not challenged by the new research.
- TB is not as easy to catch as influenza or COVID-19. Prolonged close contact with an infectious individual — typically in a shared indoor space over hours — is generally required for transmission to occur, according to CDC guidance.
- The vast majority of people exposed to TB bacteria do not develop active disease. A healthy immune system contains the bacteria in latent, non-infectious form in roughly 90 percent of exposure cases.
- Asymptomatic spread means the profile of who can transmit TB may be broader than traditional symptom-based case definitions capture — a nuance that matters for policy design, but is not a basis for generalized public alarm.
- Standard protective measures remain effective: good ventilation in shared indoor spaces, prompt testing of close contacts when a case is identified, and completing a full course of antibiotic treatment if diagnosed.
Reports of TB cases rising in some parts of the United States — with physicians warning of a rebound effect in certain communities — make the nuance of who is infectious, and when, more than an academic question. It directly informs how health departments should allocate resources for contact investigation.
Research Gaps and the Path Forward
Scientists are clear about what the field needs most: prospective cohort studies that enroll asymptomatic individuals identified through community screening and measure their actual transmission rates over time. Such studies would move the field from the correlational evidence currently available — which shows that asymptomatic people appear in transmission chains — to causal evidence about how much of the global TB burden they are responsible for generating.
Two technological advances may accelerate that work. First, exhaled-breath sampling and environmental air monitoring are being developed to directly detect viable Mycobacterium tuberculosis released by individuals, which would allow researchers to replace symptom-based infectious-status proxies with direct biological measurement. Second, rapid, low-cost TB diagnostics that do not require a patient to present with a cough — including blood-based biomarker tests and portable digital X-ray units — are in development and could reshape early case detection in high-burden settings.
Public-health agencies including the WHO are tracking the evolving evidence. Whether it ultimately triggers a formal revision of TB screening guidelines will depend on the weight of replication studies expected to emerge over the next several years. For now, the new research does what good science is supposed to do: it identifies a gap between what control programs assume and what transmission data suggest, and it points precisely toward the questions that need answering next.
The broader lesson may be one familiar from COVID-19 and influenza: that infectious diseases rarely follow the tidy, symptom-first narrative that makes them easiest to contain. Tuberculosis, which has persisted in human populations for millennia, appears to be no different.